
Robotic Retzius sparing prostatectomy
Education event Sponsored by: Intuitive Surgical
Conference Name: LIVE Operative Workshops by Intuitive
Conducted by: Intuitive Surgical India Pvt Ltd
Surgeon(s)/Speaker(s): Dr. Srivatsa N
Surgical Procedure: Urology-Robotic Radical Prostatectomy
Location: Sri Shankara Cancer Hospital & Research Centre, Bengaluru
Indexsteps
1. Genitalia and abdomen prepping and draping : The area of his genitalia and abdomen were prepped and draped in a standard fashion
2. Placing French Foley catheter : A 16-French Foley catheter was placed in the sterile field
3. Port insertion : Three Da Vinci 8-mm ports two in the Left and one in Right lower quadrants, and a 12-mm port on the Right side about 5cm away and cranial to the Right Da-vinci and a 5 mm port in between camera and 1st port were inserted.
4. Docking Robot and placing patient in steep Trendelenberg position : Once the trocars were in place, the patient was placed in steep Trendelenberg position and the robot was docked.
5. Opening Posterior peritoneum : Posterior peritoneum opened at the level of Seminal Vesicles. Vas deferens were dissected and cut laterally and Seminal vesicles were dissected
6. Dropping bladder from the anterior abdominal wall : The bladder was then dropped down from the anterior abdominal wall and the space of Retzius was entered.
7. Exposing anterior surface of the prostate and endopelvic fascia and de-fatting prostate : The anterior surface of the prostate and endopelvic fascia was exposed, and the prostate was de-fatted. The superficial dorsal vein was cauterized
8. Seperating prostate from levator ani muscles : The endopelvic fascia was incised lateral to prostate and prostate was separated from levator ani muscles.
9. Suturing Dorsal vein complex : Dorsal vein complex was then sutured with 2 - 0 V- Loc.
10. Findings : i)Mildly enlarge prostate (4 x 4 cm) ii)Enlarged bilateral pelvic lymphnodes The camera lens was converted to 30 degree down
11. Incision of anterior bladder neck : The anterior bladder neck was incised after identifying it by tug on catheter
12. Identification of foleys catheter and incision of Posterior bladder neck : The foleys catheter was identified. Balloon Deflated and catheter was brought out through the incision and was held by thread passed through the skin and Posterior bladder neck was incised completely.
13. Dissection of the posterior bladder neck and the prostate : The plane between the posterior bladder neck and the prostate was then dissected with cautery going down deep until seminal vesicals and vas were identified.
14. Exposing the lateral pedicles : Dissection done laterally exposing the lateral pedicles.
15. Lifting up on the seminal vesicals and the vas : Lifting up on the seminal vesicals and the vas, Prostate was dissected up to the rectum.
16. Swepting rectum : Rectum was then swept posteriorly off the prostate cutting Denonvilliers' fascia and was dissected comfortably with Cautry.
17. Taking Lateral pedicle with a Liga Titanium Clips : Lateral pedicle was taken with a Liga Titanium Clips and then divided.
18. Seperation of prostate from the posterior attachments : The Prostate was then separated from the posterior attachments .
19. Division of urethra : Once the apex of the prostate was cleanly dissected, The urethra was then divided at that level getting a margin around the apex of the prostate, going deep, dividing the rectourethralis.
20. Cutting Dorsal vein complex : Dorsal vein complex was then cut. And prostate was made freeing up the specimen intact.
21. Cutting margin from Bladder Neck : Specimen / Cut margin from Bladder Neck, Right pedicle margin, Left pedicle margin, Apex of the prostate was sent for frozen section – Reported as Negative.
22. Inspection of pelvis : The pelvis was carefully inspected for any bleeding
23. Dissection of Bilateral pelvic lymphnode : Bilateral pelvic lymphnode dissection done in standard manner – sent for HPR.
24. Urethrovesical anastomosis : Urethrovesical anastomosis was done using V- Loc 3 - 0 sewing around in the 6 - 12 o'clock position, working clockwise and then counter clockwise.
25. Irrigation test : Irrigation test showed no signs of leakage.
26. Insertion of Foley catheter : A new No.18 Foley catheter was inserted and balloon was inflated with 15ml sterile water.
27. Placement of surgicel : Surgicel was then placed in the right and left pelvic sidewalls.
28. Placing specimen in a bag : Haemostasis confirmed, specimen was placed in a bag.
29. Undocking robot : Robot was undocked.
30. Incision of camera port and taking prostate specimen out : The camera port incision was extended and prostate specimen was taken out with a bag through there.
31. Closing 12-mm port : The 12-mm port was closed with the No-1 PDS sutures
32. Inspecting all other port sites : All the other port sites were inspected as they were removed under direct visualization.
33. Closing of sheath : Sheath was closed with No – 1 PDS sutures
34. Closing of all the remaining skin wound sites : All the remaining skin wound sites closed with 4 – 0 Vicryl Rapide Sutures.
35. Hooking up of foley to dependent drain : The patient tolerated the procedure well. Foley was hooked up to dependent drain.
port positions
1. Prostatectomy - Port description : Procedure Performed Under GA.
Patient In Dorsal Lithotomy Position.
Small Incision Made 4cm Above The Umbilicus.
12-Mm Trocar Inserted For Camera.
Three Da Vinci 8-Mm Ports Two In The Left And One In Right Lower Quadrants, And A 12-Mm Port On The Right Side About 5cm Away And Cranial To The Right Da-Vinci And A 5 Mm Port In Between Camera And 1st Port Were Inserted As Shown In The Figure.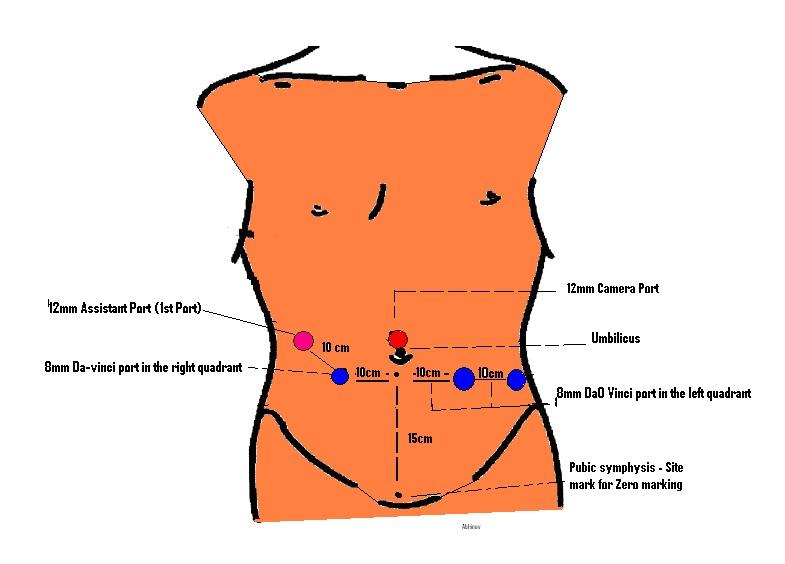
Surgical Instruments
1. Da Vinci Xi Surgical System
2. 0 and 30 deg telescope
3. Endowrist monopolar hook cautery
4. Bipolar graspers
5. Round-tip scissors
6. Needle drivers
7. Suction irrigator / suction cannula
8. Specimen retrieval bag
9. Hem-o-lock Clip
