
Lap IPOM
Surgeon(s)/Speaker(s): Dr. Lakshmi Kona
Surgical Procedure: Laparoscopic Hernia-Inguinal Hernias - TAPP (transabdominal preperiton...
Location: Yashoda Hospital, Hyderabad Somajiguda, Hyderabad
Indexsteps
1. Port placement : *10mm supra umbilical port * 5mm ports on either side * mid clavi cular port at the level of the umbilicus.
2. Create Peritoneal opening : create peritoneal opening in hockey stick fashion 2cm above the inguinal region
3. creating the preperitoneal space : creating the preperitoneal space and dilineating the hernia sac reducing the hernia sac and parietalisation of cord
4. placement of mesh : Placement of mesh and fixing to coopers ligament and conjoint muscles
5. peritoneal defect : closure of peritoneal defect
port positions
1. Port positions for Laparoscopic Hernia : Working Ports: Two. 5 mm ports on either side lateral to Rectus Sheath, in line with, or 15 degrees lower than, Umbilical Port.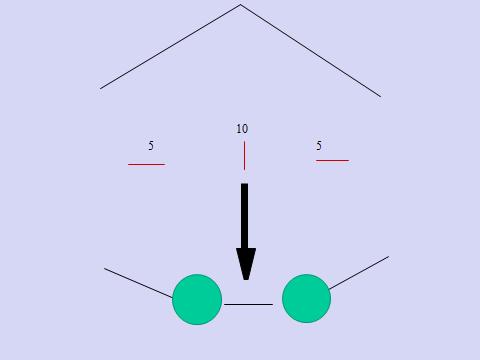
2. Port positions for Laparoscopic Hernia : Camera Port: Supra-umbilical 10mm trocar (camera port, inserted with closed technique using a Veress needle + sharp trocar or by open method)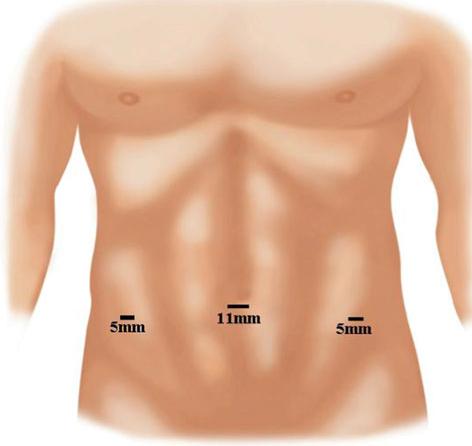
3. Working Ports : Two 5 mm ports on either side lateral to Rectus Sheath, in line with, or 15 degrees lower than, Umbilical Port.

precautionary_measures
1. First trocar : Blind entry of Veress needle and first trocar. Palmer’s point is safe entry.
2. Peritoneal incision : Peritoneal incision should not be extended medial to medial umbilical ligament as this might result in increased incidence of urinary bladder injury or bleeding from the perivesical plexus of vessels.
3. Sharp dissection in the pseudo sac : Sharp dissection in the pseudo sac area in an attempt to resect the pseudo sac may result in bleeding
4. Bladder should be drained continuously : Bladder should be drained continuously by an indwelling catheter to prevent accidental injury.
5. Separation of the sac from the cord structures : During separation of the sac from the cord structures, injury to the inferior epigastric vessels can be prevented if dissection is not continued medially beyond the level of the transversalis sling.
6. Injury to cord structures : Injury to cord structures can be prevented if the separation of the sac is performed on the upper half of the internal inguinal ring as cord structures are usually present on the inferior aspect.
7. Minimal use of monopolar or bipolar cautery : Monopolar or bipolar cautery should be used minimally as it poses a risk of injury to nerves end Vas deferens.
pre_post_measures
1. Preoperative investigations : Complete blood count:new: Blood sugar – random (fasting and postprandial, if diabetic):new: Serum creatinine:new: Liver function tests:new: Coagulation profile:new: HIV / HbsAg / Anti-HCV (if mandated by hospital):new: Blood group:new: Chest x-ray:new: ECG:new: Echocardiogram (if over 50 years):new: Abdominal ultrasound examination:new:
2. Preoperative measures : Patient is catheterized to empty the Bladder.:new: Attachment of the diathermy plate:new: Securing the patient to the table:new: Padding of the pressure points:new: Dose of prophylactic antibiotic at the time of induction of anaesthesia:new: Anti-embolic stockings / placement of an intermittent compression device on the legs:new:
3. Postoperative measures : NBM for 6 hours:new: Ambulate after that:new: Two dose of Antibiotics:new: Analgesics as required:new:
4. Warning signs in the postoperative period : Careful closure of the fascia at the umbilical trocar site:new: Infiltration of all trocar sites with local anesthetic:new: Closure of wounds and application of dressing:new: Pressure dressing is given on the Inguinal area to reduce Seroma.:new:
Surgical Instruments
1. Blunt graspers
2. 0 and 30 deg telescope
3. Fibrin glue applicator system
4. Suction irrigator / suction cannula
5. Foley catheter
6. Blunt Dissector
7. integrated trocar-dissector balloon system
8. 5 mm Trocar
9. Polypropelene Mesh
10. Mesh