
Laparoscopic Cholecystectomy
Surgeon(s)/Speaker(s): Dr. Neeraj Gupta
Surgical Procedure: Laparoscopic Cholecystectomy-Abdomen - Gall Bladder
Location: Kirloskar Hospital Hyderabad
Indexsteps
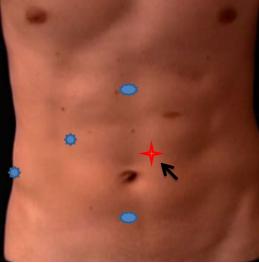
1. Insufflation and Port positioning : * Veress needle at Palmer's point * CO2 Pressures/flow rate * First 10mm port at Palmer's point * 2nd 10mm Port above and right of umbilicus * 3rd Epigastric port * 4th Right mid-axillary port
2. Retraction of the fundus : * Fundus retracted up and towards RT shoulder
3. Hertman's pouch retracted : * Hertman's pouch retracted
4. Calot's triangle dissection : * Calot's triangle dissection
5. Skeletonized Cystic duct,Clipped,Cut : * Skeletonized Cystic duct,Clipped,Cut
6. Caterpillar hump-Right hepatic artery : * Caterpillar hump-Right hepatic artery
7. Skeletonized Cystic artery,Clipped,Cut : * Skeletonized Cystic artery,Clipped,Cut
8. Dissection of GB : * GB dissected from liver bed using hook
9. Relook dissected area : * Relook dissected area
10. Specimen out : * GB extracted from LT 10mm port
11. Saline flush extraction wound : * Saline flush extraction wound
12. Sensorcaine infiltration of skin wounds : * Sensorcaine infiltration of skin wounds
port positions
1. Port positions for Cholecystectomy : * Infra-umbilical 10mm trocar (camera port, inserted with closed technique using a Verres needle + sharp trocar or by open method)
* Epigastric 10mm trocar (placed around 2cm below the edge of the liver, just to the right of the falciform ligament)
* Lateral 5mm trocar (in the anterior axillary line, used for grasping and retracting the fundus superiorly)
* Medial 5mm trocar (in the mid-clavicular line, used for lateral and downward traction on the Hartmanns pouch. The position of this critical trocar varies depending on the size of the liver and location of the gallbladder)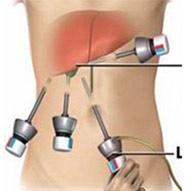
2. Port positions for Cholecystectomy : If needed 5 mm additional port for retraction on Left side of Umbilical port.
precautionary_measures
1. Precautionary Measures for this surgery : 1. For easy handling Drain GB if distended. 2. Use short bursts of energy source. 3. Keep a gauge inside helps for pressure in bleeding, good for blunt dissection. 4. Do not use Energy source near CBD. 5. Do not use CLIPS unless Critical view is clear. 6. Do not use unnecessary clips. 7. Choose right size of clip judge C duct diameter perfectly at times use ligature. 8. Collect every spilled out stone, good wash if Bile leaks.
pre_post_measures
1. Preoperative investigations : Complete blood count :new:Blood sugar – random (fasting and postprandial, if diabetic) :new:Serum creatinine :new:Liver function tests :new:Coagulation profile :new:HIV / HbsAg / Anti-HCV (if mandated by hospital) :new:Blood group :new:Chest x-ray :new:ECG :new:Echocardiogram (if over 60 years) :new:Abdominal ultrasound examination :new:MRCP / endosonography, if -Abnormal liver function tests (raised transaminases / alkaline phosphatase / ΥGT -Suspicion of bile duct stones (previous pancreatitis / obstructive jaundice)
2. Preoperative measures : Patient empties the bladder before coming to the theatre :new:Placement of a nasogastric tube :new:Attachment of the diathermy plate :new:Securing the patient to the table :new:Padding of the pressure points :new:Dose of prophylactic antibiotic at the time of induction of anaesthesia :new:Anti-embolic stockings / placement of an intermittent compression device on the legs
3. Postoperative measures : Monitoring of temperature, pulse and blood pressure :new:Allow the patient liquids after 4 – 6 hours and diet after 8 – 12 hours :new:Two more doses of antibiotics (unless an extended antibiotic therapy is required for acute cholecystitis) :new:Intravenous analgesics for the first 24 – 48 hours changed to oral analgesics at discharge :new:Anti-emetics for the first 24 hours :new:Intravenous fluids for the first 6 - 12 hours :new:Discharge once the patient is relatively pain-free, tolerating diet, ambulatory and WILLING TO GO HOME
4. Warning signs in the postoperative period : Patient feels unwell beyond the first postoperative day :new:Severe nausea / vomiting beyond first 24 hours :new:Tachycardia :new:Hypotension :new:Fever :new:Respiratory distress :new:Abdominal distension / marked tenderness / guarding / rebound tenderness / absent bowel sounds :new:Presence of bile in the drain
Surgical Instruments
1. 10mm Trocar
2. Reducer (10mm to 5 mm)
3. Fundus Grasper with Ratchet
4. Non-traumatic grasper
5. Maryland Dissector
6. Suction Irrigation canula
7. Clip applicator
8. Ultrasonic Shear
9. Port closure needle
10. Specimen retrieval bag
11. 5 mm Trocar
12. Laparoscopic Scissor
13. Electrosurgical Unit
14. Atraumatic Graspers Plain
15. L-Hook Monopolar Electrode
16. Monopolar Cautery
17. Curve Scissor Metzanbaum
18. Grasping Forceps Traumatic
19. Laparoscopic Polymer Clips